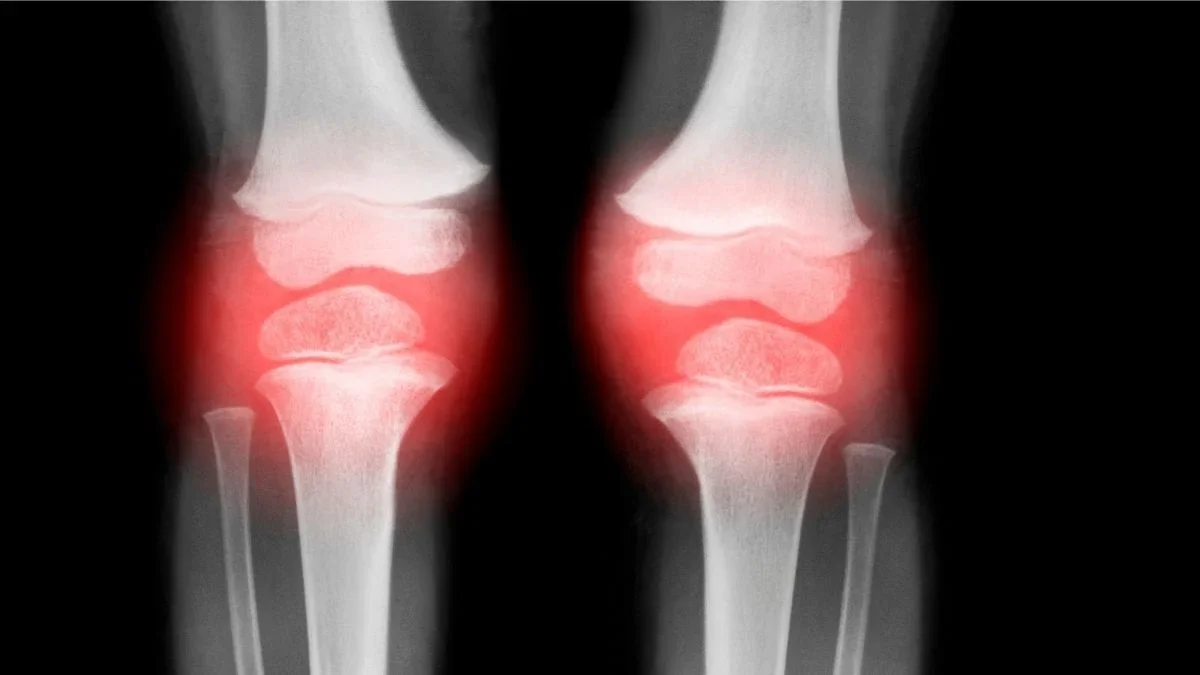
UC Boulder researchers report that a single, slow-release injection into damaged joints reversed osteoarthritis in animal models within four to eight weeks, with encouraging early tests on human cells; phase II safety/toxicity studies are planned ahead of potential human trials, though peer review is pending.
Colorado researchers report two regenerative therapies that reversed osteoarthritis signs in animals within 4–8 weeks: an injectable drug-delivery system using a repurposed FDA-approved drug and a biomaterial that recruits body-progenitor cells to repair cartilage. Backed by ARPA-H’s NITRO program with up to $33.5 million, the team has moved from phase one to phase two, with potential human trials in about 18 months and plans for commercial development through Renovare Therapeutics.
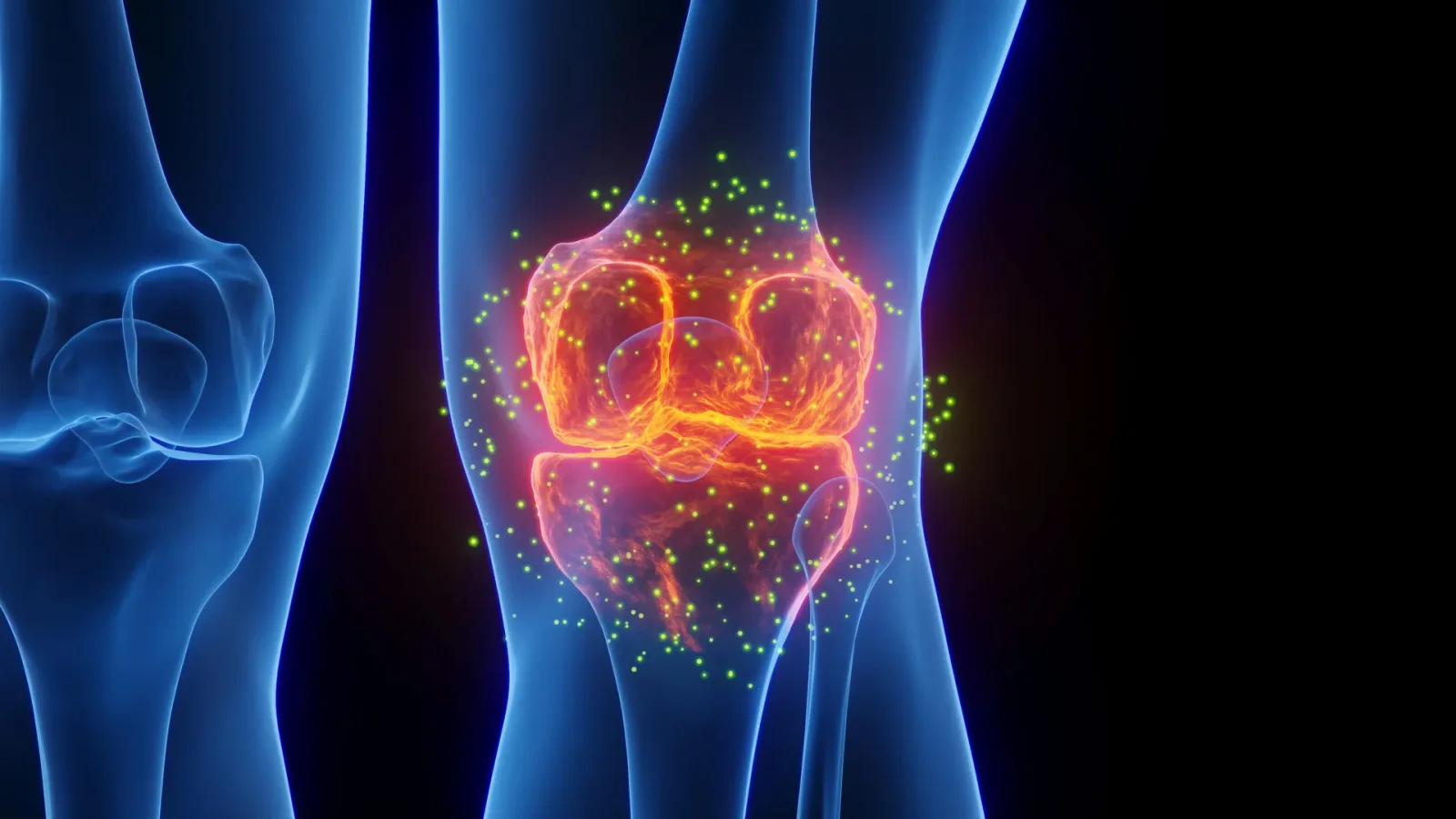
Researchers at the University of Alabama in Huntsville report that continuous low‑intensity ultrasound can shift macrophages from a pro‑inflammatory M1 state to a reparative M2‑like state, lowering inflammation and promoting tissue repair after joint injury. This non‑invasive approach could help prevent post‑traumatic osteoarthritis, with findings based on a fibronectin fragment injury model and transcriptomic analysis; however, the work is laboratory‑stage and requires animal validation before clinical use.
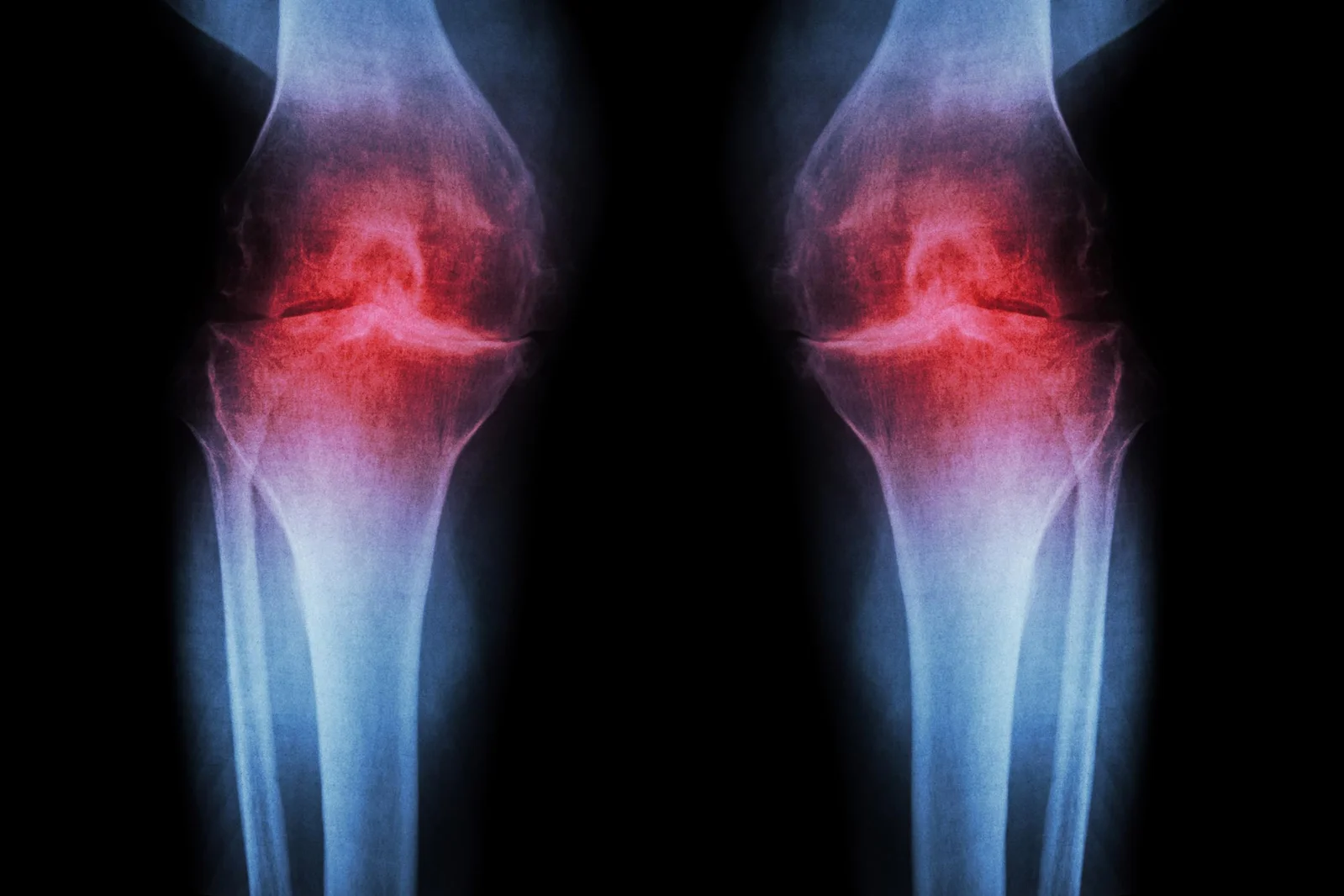
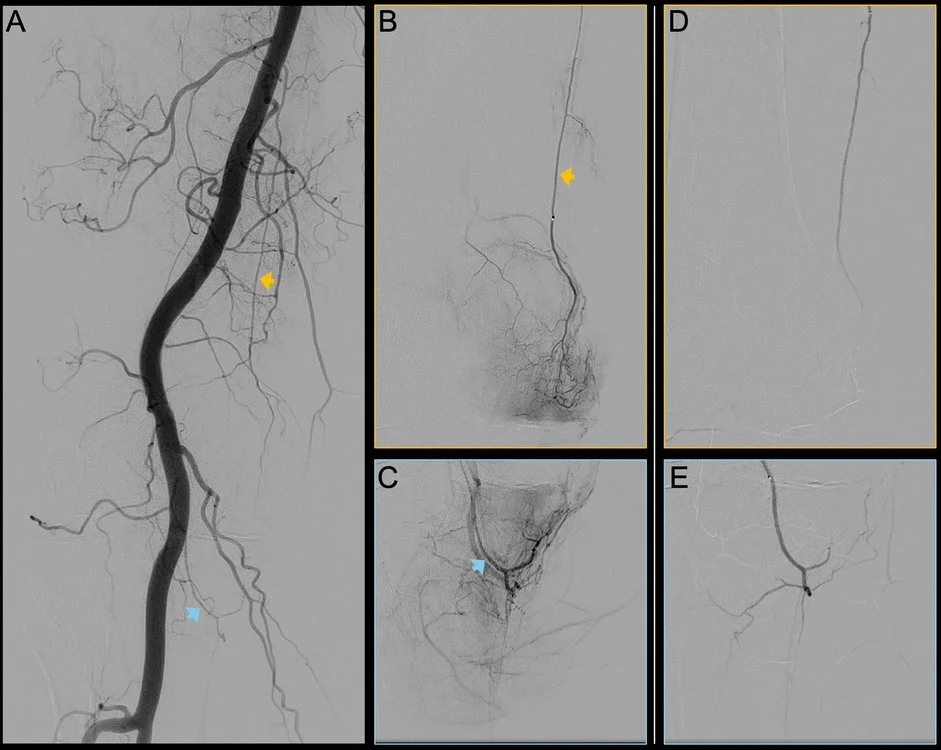
Genicular artery embolization (GAE) is an outpatient, one- to two-hour procedure that reduces inflammation by blocking blood flow to abnormal knee vessels to ease chronic knee pain from osteoarthritis. It offers a potential middle-ground between conservative treatments and total knee replacement, with about 70% of patients experiencing substantial relief and pain scores halved or better; some report no pain. Recovery is typically quick, and ongoing CU Anschutz trials are exploring long-term outcomes and broader applications beyond the knee.
A patient with severely worn knee cartilage reportedly regrew cartilage after a single injection, offering a non-surgical alternative to knee replacement and signaling a potential shift in how osteoarthritis is treated.
Genicular artery embolization (GAE), a minimally invasive procedure that injects resorbable gelatin microspheres to block abnormal knee vessels, aims to reduce inflammation and pain in osteoarthritis. In a real-world study of 194 participants (average age ~69), most experienced significant pain relief and improved function for at least 12 months, with 80% surpassing the minimum clinically important difference; about 23% needed a second GAE, and adverse events were mild and limited to 6.7% of participants. The treatment offers a potential middle option between injections and joint replacement.
Blocking the aging-related enzyme 15-PGDH reprograms existing cartilage cells to regrow hyaline cartilage in aged mice and human knee tissue, prevents osteoarthritis after ACL-type injuries, and could be delivered by injection or an oral drug; the approach might reduce the need for joint replacements if proven in people, and related clinical trials for the inhibitor are already underway for other aging-related conditions; researchers note the regeneration comes from changing existing chondrocytes rather than stem cells, and there are patent/licensing ties involved.
The largest umbrella review of collagen research (nearly 8,000 participants across 113 randomized trials) finds collagen supplements can improve skin hydration and elasticity and reduce osteoarthritis pain with longer use; modest improvements in muscle and tendon structure; little evidence for enhanced athletic performance or recovery; mixed or inconclusive results for metabolic and dental health; overall, collagen may support healthy aging but is not a quick fix for sports performance, and more high-quality trials are needed.
A US study of 6.8 million knee-osteoarthritis patients found that GLP-1 weight‑loss drugs—especially three years of treatment with semaglutide or tirzepatide—were associated with meaningful reductions in knee-replacement risk, potentially preventing thousands of surgeries annually in the US and UK if widely adopted. The observed benefits increased with longer treatment, but experts caution these drugs are not OA-approved and the study shows association, not causation.
In animal studies, two regenerative approaches—a single injectable that releases medication over months and a biomaterial scaffold that recruits body’s progenitor cells—repaired damaged cartilage and bone within 4–8 weeks, with ARPA-H funding advancing the project toward clinical trials in about 18 months, aiming for affordable, minimally invasive, single-visit therapies that could eventually reduce the need for joint replacement.
New evidence suggests regular, guided physical activity should be a first-line treatment for osteoarthritis to reduce pain and improve mobility, often outperforming temporary fixes like drugs or injections. While some patients are steered toward surgery, many benefit from supervised exercise that strengthens the whole joint and may lower systemic inflammation. Aerobic activities such as brisk walking, swimming, or cycling tend to yield the largest short-term pain relief, with yoga, tai chi, pilates, and resistance training also helping. The key is a sustainable, professionally guided plan—the best type of exercise is the one a person can consistently do—to manage symptoms and potentially reduce the need for invasive procedures over the long term.
Researchers have identified the SHP (NR0B2) protein as a key defender of cartilage whose levels fall as osteoarthritis progresses. Restoring SHP in animal models reduced cartilage damage, improved joint function, and dampened cartilage-degrading enzymes (MMP-3 and MMP-13) via the IKKβ/NF-κB pathway. Gene delivery of SHP into affected joints produced lasting benefits, suggesting a potential disease-modifying approach to slow or halt osteoarthritis.
Ten-year follow-up of the FIDELITY randomized trial shows arthroscopic partial meniscectomy offers no functional or pain benefit versus sham for degenerative meniscal tears and may accelerate osteoarthritis progression; more patients in the surgical group required knee replacement or high tibial osteotomy. The findings, aligning with prior 1- and 5-year data, argue against using APM in this patient population except in specific acute or mechanical cases.
Stanford researchers identify the protein 15-PGDH as a driver of age-related cartilage breakdown and show that blocking it can thicken worn knee cartilage and reprogram existing chondrocytes, reversing degeneration in older mice and regenerating cartilage in human tissue, signaling potential clinical trials and a possible path to avoiding joint replacement.
Stanford researchers showed that inhibiting the aging-related enzyme 15-PGDH reverses cartilage aging in mice, regenerating cartilage and improving gait; human knee tissue also exhibits regeneration signs, suggesting a potential new osteoarthritis therapy with clinical trials possible within 18 months, and crucially without relying on stem cells.